A Very Wise Sage Once Told Me Fitness is 80% Diet.
Having worked in and around gym’s for the last 16 years I have have worked with fitness professionals, body builders and athletes. I have also endured my own journey towards fitness and seen many patients change their physique. It’s no secret diet and exercise are the cornerstones of fitness. For me the holy grail of fit was more raw foods and high intensity interval training or metabolic training. Real changes are those that transcend your schedule and lifestyle, which brings me to my next statement.
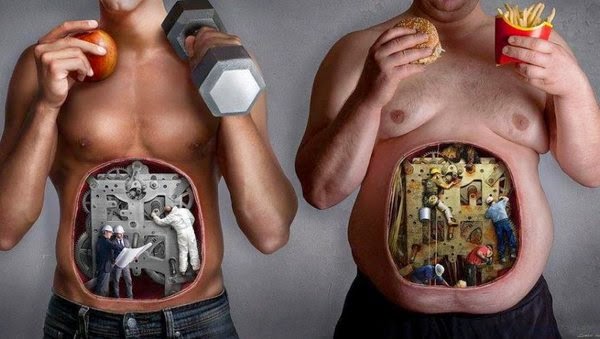
You MUST Change How You View Food.
Our ancestors must have gotten a completely different palate, keeping in mind that spices were reserved for the privileged. Food was most likely bland and it was most certainly sparse, my parents grew up in German occupied Greece and even one generation ago, there were people starving to death. The take home point is that it’s only until recently that our culture has put so much emphasis on eating as a social event. Historically food has been viewed as fuel.

Dinner and Drinks?
I have many patients and friends who ask how to improve their body composition(less fat or more muscle), and inevitably the conversation moves to dinning. Going out to dinner has become a common pastime and a weekly occurrence. The individual looses control of the preparation of the food and seldom asks for nutritional information, since they’re going out, one may figure “where’s the fun in that?” The problem is that just an appetizer alone can account for all of your daily allowance of fat and calories as explained in this Good Morning America post. Add a few beers or glasses of wine at around 150 calories each and you can see even a modest meal turns into a 4000 calorie event.
 |
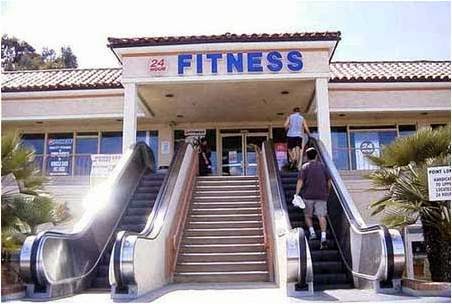
| Convenient, but obese kids make obese adults. |
The Good News? We’re Not the Fattest Country Anymore!
Mexico has surpassed the U.S. as the fattest country in the world, perhaps due to the infiltration of Starbucks. All kidding aside, our super-sized portions and Mocha-chino Grande (600 calories) have consistently ranked us among the fattest in the world. A simple way to lose excess weight is to steer clear of drinking calories.
Prepare for the End – the Bottom End of Course.
Food preparation sounds like a big task, but it doesn’t need to be. Baking 5 or 10 chicken breasts at the beginning of the week can give you all of the salad with chicken all week. Boiling 2 dozen eggs, also an excellent protein rich and calorie poor option for breakfast or snack. Put some broccoli florets in a zip-lock and grab some hummus for a balanced, low calorie filling snack! Greek yogurt is one of the packaged foods that you can eat and feel great about. There are tons of great ideas in magazines and online, but the sooner you appreciate the power of preparing your meals the faster you’ll be feeling and looking great.
Diets Don’t Work–You Need a Lifestyle Change
Understanding this is a total shift in how to live and not a diet. Gradual changes are ones that cause less stress and will be more sustainable. Limiting half of the starchy carbohydrate that you typically eat at a sitting will be a great stepping stone to eventually eliminating them altogether. Gluten and sugar have a major impact on inflammation, insulin levels and cardiovascular health. Dr. Seaman did an interview that can be found here explaining how our diet is killing us slowly.
It’s better to look good than to feel good
Looking good and feeling good are very much intertwined, in explaining the way to a fitter physique we also extoll the benefits of good health. Not everyone wants a beach body and by following some of the guidelines we have set forth, will not only get you looking better but also improve your cholesterol and triglyceride counts. It’s important to keep in mind why we would want to change, it’s not all about aesthetics.
 |
| You look marvelous darling |
Everything in Moderation
We all enjoy a night out and if you’re active and practicing good eating habits most of the time you can enjoy a nice restaurant, but overall, most may want to develop other forms of entertainment. Active hobbies would have a definite impact, increasing activity levels as well as limiting outside meals. Personally, my wife and I have shed our inhibitions and frequently dance like no one is watching in a club full of people way younger(at least chronologically).
Today
we provided principles, so you can adapt your own protocols, don’t
hesitate to contact us with questions.
Please let us know you visited our blog by liking, commenting & sharing.

Specialist. He lives and works in the Exton PA area and has devoted
himself to furthering his understanding of movement related disorders.
He teaches continuing education and operates a private practice. More
information can be found at Kinetx.org and feel free to like us at our facebook page.









































{kind=link}